Dental Benefits
All eligible Associates can elect comprehensive dental coverage through Ameritas. This plan is voluntary and is 100% paid for by the Associate.
Dental Benefit Comparison
| Plan Features | Dental PPO Ameritas Classic Network |
|||
|---|---|---|---|---|
| In-Network | Out-of-Network | |||
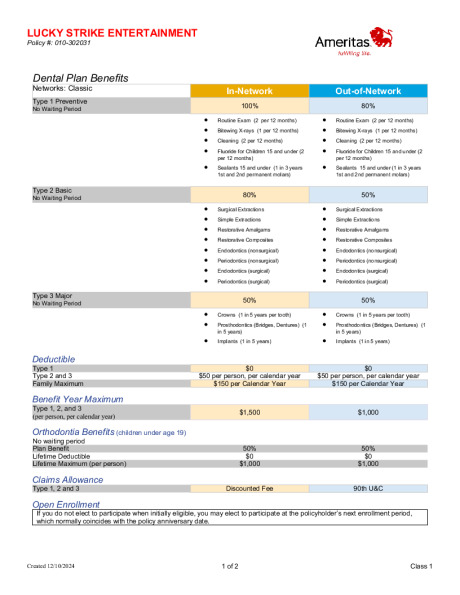
| Annual Deductible | ||||
| Individual | $50 | $50 | ||
| Family | $150 | $150 | ||
| Waived for Preventive Care? | Yes | Yes | ||
| Annual Maximum | ||||
| Per Person | $1,500 | $1,000 | ||
| Preventive Exam, X-Rays, Sealants, Fluoride for Children under age 15 |
No cost | 20% coinsurance | ||
| Basic Fillings, Root Canals (Endodontic Care), Periodontal Scaling, Minor Oral Surgery, Simple Extractions |
20% after deductible | 50% coinsurance | ||
| Major Crowns, Dentures, Implants, Onlays, Fixed Bridges, Denture Repairs |
50% after deductible | 50% after deductible | ||
| Orthodontia | ||||
| Benefit Percentage | 50% coinsurance | 50% coinsurance | ||
| Adults | Not covered | Not covered | ||
| Dependent Child(ren) | Covered to age 19 | Covered to age 19 | ||
| Lifetime Maximum | $1,000 | $1,000 | ||
| Benefit Waiting Periods | 0 months | 0 months | ||
Dental Contributions
| Dental (Pre-Tax Contributions) | ||||
|---|---|---|---|---|
| Weekly Premiums | Bi-Weekly Premiums | |||
| Associate | $5.19 | $10.39 | ||
| Associate + Spouse | $11.74 | $23.48 | ||
| Associate + Child(ren) | $10.39 | $20.77 | ||
| Associate + Family | $17.81 | $35.61 | ||