Vision Benefits
Vision Insurance is available through Ameritas. During the enrollment process, you will have the option of utilizing either the VSP Network or the EyeMed network. This plan is voluntary and is 100% paid for by the Associate.
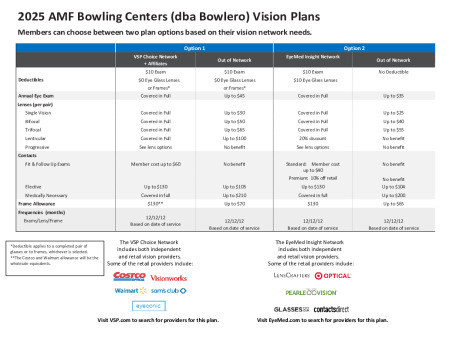
You must choose the network you wish to participate in. Once your decision has been made during enrollment, that is the network you will continue to participate in for the remainder of the plan year.
Vision Plan Comparison
| Plan Features | Vision Plan | ||||||
|---|---|---|---|---|---|---|---|
| EyeMed Network | EyeMed Out-of-Network | VSP Network | VSP Out-of-Network | ||||
| Deductible | $10 Exam $10 Eye Glass Lenses |
No deductible | $10 Exam $0 Eye Glass Lenses or Frames* |
$10 Exam $0 Eye Glass Lenses or Frames | |||
| Annual Eye Exam | Covered in full | Up to $35 | Covered in full | Up to $45 | |||
| Lenses (per pair) Single Vision Bifocal Trifocal Lenticular Progressive |
Covered in full Covered in full Covered in full 20% discount See Lens Options |
Up to $25 Up to $40 Up to $55 No benefit N/A |
Covered in full Covered in full Covered in full Covered in full See Lens Options |
Up to $30 Up to $50 Up to $65 Up to $100 N/A | |||
| Contacts Fit & Follow-up Exams Standard Premium (Allowance) Elective Medically Necessary |
Member cost up to $40 10% off of retail Up to $130 Covered in full |
No benefit No benefit Up to $104 Up to $200 |
Member cost up to $60 Member cost up to $60 Up to $130 Covered in full |
No benefit No benefit Up to $105 Up to $210 | |||
| Frame Allowance | $130 | Up to $65 | $130** | Up to $70 | |||
| Frequencies (months) Exam / Lens / Frame |
12 / 12 / 12 Based on date of service |
12 / 12 / 12 Based on date of service |
12 / 12 / 12 Based on date of service |
12 / 12 / 12 Based on date of service | |||
Note: *Deductible applies to a complete pair of glasses or to frames, whichever is selected. **The Costco and Walmart allowance will be the wholesale equivalent.
Vision Contributions
| Vision (Pre-Tax Contributions) | ||||
|---|---|---|---|---|
| Weekly Premiums | Bi-Weekly Premiums | |||
| Associate | $1.26 | $2.52 | ||
| Associate + Child(ren) | $2.82 | $5.63 | ||
| Associate + Spouse | $2.41 | $4.82 | ||
| Associate + Family | $3.99 | $7.98 | ||